The goal of breast reconstruction is to restore one or both breasts to near normal shape, appearance, symmetry and size following mastectomy, lumpectomy or congenital deformities.
Breast reconstruction often involves multiple procedures performed in stages and can either begin at the time of mastectomy or be delayed until a later date.
Breast reconstruction generally falls into two categories: implant-based reconstruction or flap reconstruction. Implant reconstruction relies on breast implants to help form a new breast mound. Flap (or autologous) reconstruction uses the patient's own tissue from another part of the body to form a new breast.
There are a number of factors that should be taken into consideration when choosing which option is best:
- Type of mastectomy
- Cancer treatments
- Patient's body type
A note about symmetry
If only one breast is affected, it alone may be reconstructed. In addition, a breast lift, breast reduction or breast augmentation may be recommended for the opposite breast to improve symmetry of the size, shape and position of both breasts.
Breast reconstruction is a highly individualized procedure. You should do it for yourself, not to fulfill someone else's desires or to try to fit any sort of ideal image.
You may be a candidate for breast reconstruction if:
- You are able to cope well with your diagnosis and treatment
- You do not have additional medical conditions or other illnesses that may impair healing
- You have a positive outlook and realistic goals for restoring your breast and body image
Although breast reconstruction can rebuild your breast, the results are highly variable:
- A reconstructed breast will not have the same sensation or feel as the breast it replaces
- Visible incision lines will always be present on the breast, whether from reconstruction or mastectomy
- Certain surgical techniques will leave incision lines at the donor site, commonly located in less exposed areas of the body such as the back, abdomen or buttocks
Breast reconstruction recovery
Following your breast reconstruction surgery for flap techniques and/or the insertion of a breast implant, gauze or bandages may be applied to your incisions.
An elastic bandage or support bra will minimize swelling and support the reconstructed breast. A small, thin tube may be temporarily placed under the skin to drain any excess blood or fluid.
You will be given specific instructions that may include: How to care for your surgical site(s) following surgery, medications to apply or take orally to aid healing and reduce the risk of infection, specific concerns to look for at the surgical site or in your general health and when to follow up with your plastic surgeon.
Be sure to ask your plastic surgeon specific questions about what you can expect during your individual recovery period.
- Where will I be taken after my surgery is complete?
- What medication will I be given or prescribed after surgery?
- Will I have dressings/bandages after surgery? When will they be removed?
- Will there be drains? For how long?
- When can I bathe or shower?
- When can I resume normal activity and exercise?
- When do I return for follow-up care?
Healing will continue for several weeks while swelling decreases and breast shape/position improve. Continue to follow your plastic surgeon’s instructions and attend follow-up visits as scheduled.
Breast reconstruction results
The final results of breast reconstruction following mastectomy can help lessen the physical and emotional impact of mastectomy.
Over time, some breast skin sensation may return, and scar lines will improve, although they will never disappear completely.
There are trade-offs, but most women feel these are small compared to the large improvement in their quality of life and the ability to look and feel whole.
Careful monitoring of breast health through self-exam and other diagnostic techniques is essential to your long-term health.
When you go home
If you experience shortness of breath, chest pains or unusual heartbeats, seek medical attention immediately. Should any of these complications occur, you may require hospitalization and additional treatment.
The practice of medicine and surgery is not an exact science. Although good results are expected, there is no guarantee. In some situations, it may not be possible to achieve optimal results with a single surgical procedure, and additional procedures may be necessary.
Be careful
Following your physician's instructions is key to the success of your surgery. It is important that the surgical incisions are not subjected to excessive force, abrasion or motion during the time of healing. Your doctor will give you specific instructions on how to care for yourself.
Breast reconstruction procedure steps
A breast reconstruction procedure includes the following steps:
Step 1 – Anesthesia
Medications are administered for your comfort during the surgical procedure. The choices include intravenous sedation and general anesthesia. Your doctor will recommend the best choice for you.
Step 2 – Flap techniques reposition a woman's own tissue to create or cover the breast mound
Sometimes a mastectomy or radiation therapy will leave insufficient tissue on the chest wall to cover and support a breast implant. In these cases, breast reconstruction usually requires either a flap technique or tissue expansion.
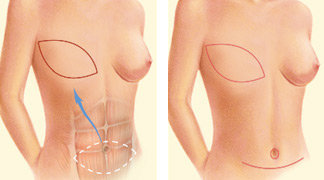
A TRAM flap uses donor muscle, fat and skin from a woman's lower abdomen to reconstruct the breast. The flap may either remain attached to the original blood supply and be tunneled up through the chest wall, or be completely detached, and formed into a breast mound.
Alternatively, your surgeon may choose the DIEP flap or SIEA flap techniques, which do not use abdominal muscle but transfer only skin and fat to the chest from the abdomen. If there is insufficient tissue on the lower abdomen, other donor sites such as the buttocks or thighs may be selected (SGAP flap, TUG flap, PAP flap).
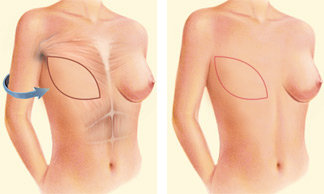
A latissimus dorsi flap uses muscle, fat and skin from the back tunneled to the mastectomy site and remains attached to its donor site, leaving blood supply intact.
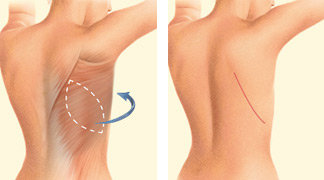
Occasionally, the flap can reconstruct a complete breast mound, but often the latissimus flap provides the muscle and tissue necessary to cover and support a breast implant.
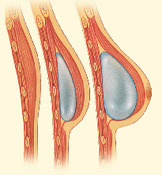
Step 3 – Tissue expansion stretches healthy skin to provide coverage for a breast implant
For women who do not require breast radiation and would like to avoid a separate donor site, implant-based reconstruction is an option. Reconstruction with tissue expansion allows an easier recovery than flap procedures, but it can be more lengthy reconstruction process.
It usually requires several office visits over 1-2 months after placement of the expander to gradually fill the device with saline through an internal valve to expand the skin. Newer air-filled devices may allow patient-controlled expansion at home using a remote dosage controller.
A second surgical procedure will be needed to replace the expander if it is not designed to serve as a permanent implant.
 Step 4 – Surgical placement of a breast implant creates a breast mound
Step 4 – Surgical placement of a breast implant creates a breast mound
A breast implant can be an addition or alternative to flap techniques. Surgeons may also use an implant as a temporary placeholder during other breast cancer treatments until you are ready for more involved flap reconstruction techniques. Saline and silicone implants are available for reconstruction.
Your surgeon will help you decide what is best for you. Reconstruction with an implant alone usually requires tissue expansion. Direct-to-implant breast reconstruction may be an option for some women undergoing mastectomy with certain tumor characteristics and breast shapes.
Step 5 – Reconstructing a nipple and areola, breast revision techniques
For women who are not candidates for nipple-sparing mastectomy, breast reconstruction is completed through a variety of techniques that reconstruct the nipple and areola. Techniques usually involve folding skin to create the shape of a nipple followed by tattooing. Three-dimensional nipple-areolar tattooing may be used alone to create the appearance of a realistic nipple with the illusion of projection. Breast reconstruction outcomes can often be enhanced with staged revision procedures that improve symmetry, use liposuction with fat grafting and improve the appearance of the donor site.
Breast reconstruction risks and safety
The decision to have breast reconstruction surgery is extremely personal. You'll have to decide if the benefits will achieve your goals and if the risks and potential complications are acceptable.
Your plastic surgeon and/or staff will explain in detail the risks associated with surgery. You will be asked to sign consent forms to ensure that you fully understand the procedures you will undergo and any risks or potential complications. The decision to pursue breast reconstruction does not change your risk of breast cancer recurrence.
The possible risks of breast reconstruction include, but are not limited to, bleeding, infection, poor healing of incisions and anesthesia risks. You should also know that:
- Flap surgery includes the risk of partial or complete loss of the flap and a loss of sensation at both the donor and reconstruction site.
- The use of implants carries the risk of breast firmness (capsular contracture) and implant rupture.
Breast implants do not impair breast health. Careful review of scientific research conducted by independent groups such as the Institute of Medicine has found no proven link between breast implants and autoimmune or other systemic diseases.
Information on Breast Implant-Associated ALCL
Visit breastimplantsafety.org for current information.
Where will my surgery be performed?
Surgery for your breast reconstruction is most often performed in a hospital setting, possibly including a short hospital stay, and your doctor will likely use general anesthesia. Some follow-up procedures may be performed on an outpatient basis, and local anesthesia with sedation may be used. These decisions will be based on the requirements of your specific procedure and in consideration of your preferences and your doctor's best judgment.